Shoulder Injuries: Rotator Cuff

Bony Anatomy:
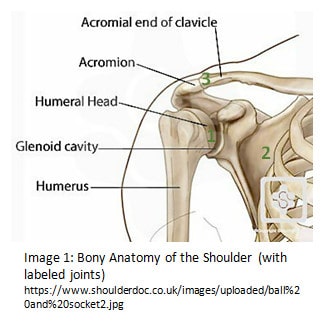
The shoulder is comprised of four joints made up of several bones (see Image 1). These joints are the glenohumeral (1), scapulothoracic (2), acromioclavicular (3), and sternoclavicular (not shown). For the sake of this article, we’ll focus primarily on the glenohumeral joint, where the humerus (upper arm bone) attaches to the scapula (shoulder blade). The rotator cuff muscles work at this joint and it is the joint that most people associate with the “shoulder.”
With the glenohumeral joint, it is important to note how incongruent the bones are: the head of the humerus sits in the glenoid fossa (the small cup-like structure on the scapula) like a golf ball on a tee. This allows for the great mobility of this joint, however it requires soft tissue structures like muscles and ligaments to make up for the lack of bony stability.
Soft Tissue Anatomy:
Take a look at Image 2.To orient you, this is looking at a right shoulder from the side, with the humerus taken out. All of the labeled structures provide congruency for the glenohumeral joint that it lacks in bony anatomy alone. The shoulder joint has three methods of stabilization: suction, static, and dynamic. The dark blue circle labels the glenoid labrum. The labrum is a ring of connective tissue surrounding the glenoid that provides a suction-like force to keep the humeral head in the glenoid. The static stabilizers of the shoulder are the ligaments that support the humeral head and keep it from dislocating, indicated by the light blue circles. The shoulder is dynamically stabilized by the rotator cuff muscles, which are circled in orange.
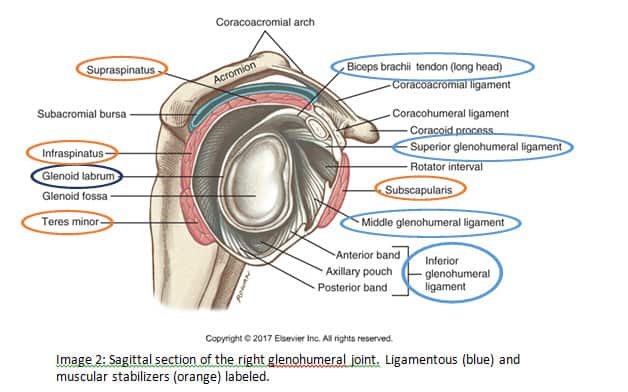
It is important to understand that the rotator cuff muscles are the only contractile tissues stabilizing the humeral head, which means that they are the only structures that can actively react to changes in shoulder position. The labrum and the ligaments can stretch to accommodate movement and have an elastic quality that allows them to ‘rebound’ to their original length, but this is not the same as a muscle contraction. Understanding this distinction sheds light as to how overuse injuries occur.
Overuse Injuries
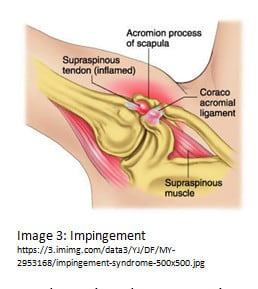
There are two major overuse injuries that occur: shoulder impingement and rotator cuff tears. Both can be caused by traumatic events as well, but we will focus more on overuse or repetitive movements as the cause of dysfunction.
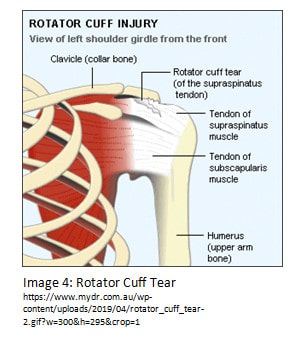
Rotator cuff tears (see Image 4) occur by repetitive shoulder movements, most commonly in overhead athletes or people who perform continuous work overhead. In and overhead position, the rotator cuff must work harder to ensure stability of the shoulder joint. With overhead athletes, the rotator cuff must operate at its outer limits frequently, which puts immense stress on the muscles. Because these muscles are the only structures actively stabilizing dynamic movements of the arm, consistent strenuous work with inadequate rest can lead to tears, either partial or complete.
Sometimes these two injuries are concurrent, but regardless of which injury is sustained, the impairments experienced are typically the same. People with these injuries have pain and limited motion when reaching overhead and with repetitive arm movements, weak external rotation strength, and have trouble with activities such as washing their hair, tucking in shirts, and/or pushing and pulling tasks. Aside from a traumatic onset, these injuries usually manifest as increasing pain over weeks or months after performing overhead/repeated activities that becomes constant and ultimately limits function.
Prevention
So, what can we do to avoid overuse injuries? One way is to create variability of movements throughout the day; that is to say, avoid doing the same repetitive task continuously. Try to break it up by taking rests every 30-60 minutes, and/or use your arm differently throughout the day. For those whose situations are less flexible, starting an appropriate and progressive strength and mobility training regimen can help strengthen the rotator cuff to perform better or for longer. I cannot stress enough the importance of having appropriate technique when performing exercises. Poor technique can lead to less
Not only should the rotator cuff be trained, but other muscles controlling the shoulder should be adequately strengthened as well. The pectoralis, latissimus, rhomboids, and trapezius play a role in how the shoulder stabilizes and moves. It is important to train both for strength as well as motor control, as these muscles tend to be the ones that compensate for weak rotator cuff muscles.
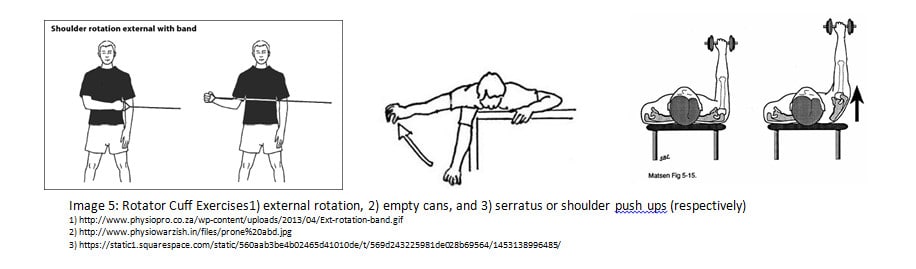
The three most common exercises for the rotator cuff and shoulder stability are 1) external rotation, 2) empty cans, and 3) serratus or shoulder pushups (see Image 5 below).
If you or someone you know has a rotator cuff tear or impingement, the first step is usually conservative treatment. A primary care provider may take imaging (x-rays, MRIs, etc.) to understand the extent of the injury, and commonly refers out to physical therapy. In physical therapy, pain management and movement training are initiated to allow for appropriate tissue healing and safe strengthening to prevent future injury. If conservative treatment fails or the injury is severe, surgery may be an option. Surgeons can fix a tear and/or increase the space between the humerus and acromion to eliminate pinching. Physical therapy is recommended after surgery as well to promote optimal tissue healing and strengthening to prevent future injury.
Depending on severity, people receiving care for overuse injuries can return to normal activities in about four to six months. Tendons and ligaments may take up to 10-12 months to return to 90% of their original strength, so patients should continue to rehabilitate even after discharge from physical therapy and return to prior level of function gradually.
Rotator cuff injuries are common in all age groups and can have a serious impact on arm function and quality of life. Prevention through appropriate exercise and a healthy lifestyle are integral for anyone participating in repetitive and/or overhead activities. If someone does sustain an injury, physical therapy (and sometimes surgery) can get them back to function in a reasonable amount of time. These injuries are some of the most commonly researched and treated, and health professionals are more than prepared to treat any dysfunction. The key is to work on prevention strategies and check in with a health care provider at the first suspicion of dysfunction. Now, who’s up for a game of catch?
Sources:
- Codsi M, Howe CR. Shoulder Conditions. Physical Medicine and Rehabilitation Clinics of North America. 2015;26(3):467-489. doi:10.1016/j.pmr.2015.04.007.
- DynaMed Plus [Rotator Cuff Impingement]. Ipswich (MA): EBSCO Information Services. http://www.dynamed.com. Accessed October 10, 2010
- Oliva F, Piccirilli E, Bossa M, et al. I.S.Mu.L.T – Rotator Cuff Tears Guidelines. Muscles, Ligaments and Tendons Journal. 2015;5(4):227-263. doi:10.11138/mltj/2015.5.4.227.
- Sambandam SN, Khanna V, Gul A, Mounasamy V. Rotator cuff tears: An evidence based approach. World Journal of Orthopedics. 2015;6(11):902-918. doi:10.5312/wjo.v6.i11.902.
- Breazeale, N M (04/1997). “Partial-thickness rotator cuff tears. Pathogenesis and treatment.”. The Orthopedic clinics of North America (0030-5898), 28 (2), 145.
- Kadi R, Milants A, Shahabpour M. Shoulder Anatomy and Normal Variants. Journal of the Belgian Society of Radiology. 2017;101(S2):3. doi:10.5334/jbr-btr.1467.