Plantar Fasciitis

These risk factors will make more sense as we delve into the anatomy and pathology of plantar fasciitis, and we will also talk about different ways to deal with and prevent plantar fasciitis in this article. Let’s get to it!
Plantar Fasciitis
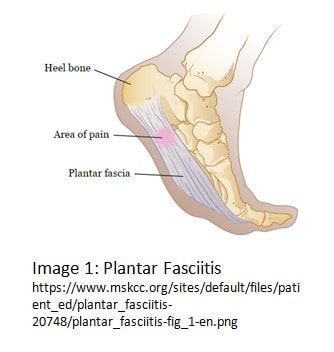
Let’s break down “plantar fasciitis”: plantar refers to the foot, specifically the bottom of the foot; fascia is the term for the connective tissue that makes up the arch of the foot; -itis refers to inflammation, or irritation of tissue. There we have it: there is inflammation in the bottom of the foot, and it [typically] causes pain. Image 1 provides a visual.
Because of the way that the plantar fascia attaches to the foot, it is stretched during toe-off, when the big toe is in extension (similar to the foot position in Image 1). Therefore high-impact activities that require a more powerful and frequent push-off can lead to microtears in the fascia. Fascia is mobile, but not elastic, meaning that it is not intended to stretch and recoil. One of the important functions of fascia is to maintain its tension in order to support the arch of the foot in various positions. Repeated tensile forces on the fascia can compromise that support through excessive lengthening (no recoil, so the fascia remains too long) or mircotearing.
A person is more likely to develop plantar fasciitis if they have multiple risk factors; for example, a runner with inappropriate shoes and limited ankle motion is more at risk than someone with a single risk factor alone.
All of the risk factors associated with plantar fasciitis compromise the mechanics of the foot during locomotion and create additional strain on the fascia.
The location of pain with plantar fasciitis is typically closer to the heel. This is the thinnest area of the plantar fascia, making it more susceptible to tearing when put under excessive load. It is normal for people to experience the most pain with the first couple of steps in the morning, and increased pain again during and after weightbearing activity (standing, walking, running). Symptoms can be present for six months or more, however, there are several ways to treat and prevent plantar fasciitis to decrease that time.
Treatment
There are a number of ways to treat plantar fasciitis: the most popular to do on one’s own are strengthening, stretching, and orthoses. Strengthening of the intrinsic foot muscles and calf can help with foot mechanics during gait, as well as improve ankle motion and stability. Stretching the fascia and the calf muscles are also good ways to manage symptoms, as the length of the fascia can be changed with sustained holds. This may be helpful in people with higher arches, as their fascia has additional tension that predisposes them to plantar fasciitis. Providing additional length to the tissue through controlled stretching may allow for a more optimal fascial tension during activity. Orthoses (also called “inserts”) can correct structural or functional arch deformities, and/or provide more support or absorption depending on what is required. A physical therapist or podiatrist can give appropriate shoe and orthosis recommendations.
Physical therapy is another option for plantar fasciitis treatment. Physical therapists (PTs) are equipped to accurately rule in or out plantar fasciitis as the cause of foot pain and treat it appropriately. Strengthening and stretching are typical aspects of treatment, as are various manual techniques to improve nerve function, decrease pain, and increase range of motion of the ankle and foot. When prescribed by a physician, PTs are also qualified to apply iontophoresis, a method of applying medication, in this case to the sole of the foot, through electrical current. Iontophoresis is known to be very effective when combined with taping over 6 treatments.
Conservative treatment is often effective, however there is the rare chance that surgical intervention is warranted. In such procedures, an orthopedic surgeon will “release” the plantar fascia. This “release” essentially cuts the fascia to reduce the amount of tension. While people end up with pain relief, rehabilitation is required to strengthen the muscles within the foot to make up for the loose fascia. It is common for people who have this procedure to develop arthritis in the midfoot region later in life.
Prevention
A lot of the techniques used in conservative treatment can also be used as prevention. Maintaining ankle range of motion by stretching the calves and ensuring the use of appropriate footwear and/or orthoses during weightbearing activities are simple ways to prevent plantar fasciitis and continue doing the activities you love. It is also important to utilize an appropriate training program: performing high level activity after a period of inactivity or progressing running speed or distance too quickly could lead to plantar fasciitis. PTs, and some personal trainers with experience training runners can help ensure that a running program is properly progressed.
Plantar fasciitis is a common condition experienced by the athletic population. It occurs when multiple factors compromise the mechanics of how the foot absorbs and transfers force during high intensity activity, such as running. Maintaining appropriate strength and motion and ensuring the use of well-fitted footwear and a properly progressed training program can prevent plantar fasciitis. For people in the sedentary population who experience plantar fasciitis, there is limited evidence that maintaining a BMI within the normal range will aid in reducing symptoms. While plantar fasciitis can be painful, there are several effective conservative treatments to heal the tissue and return full function in order to continue participation in desired activities.So, keep calm and run on!
Sources:
- Martin RL, Davenport TE, Reischl SF, et al. Heel Pain—Plantar Fasciitis: Revision 2014.J Orthop Sports Phys Ther. 2014;44(11):A1-A23. doi:10.2519/jospt.2014.0303
- Plantar Fasciitis. (2019, June 25). Physiopedia. Retrieved 23:46, July 23, 2019 from https://www.physio-pedia.com/index.php?title=Plantar_Fasciitis&oldid=215416.